Obturator Internus, Piriformis & the Pudendal Nerve
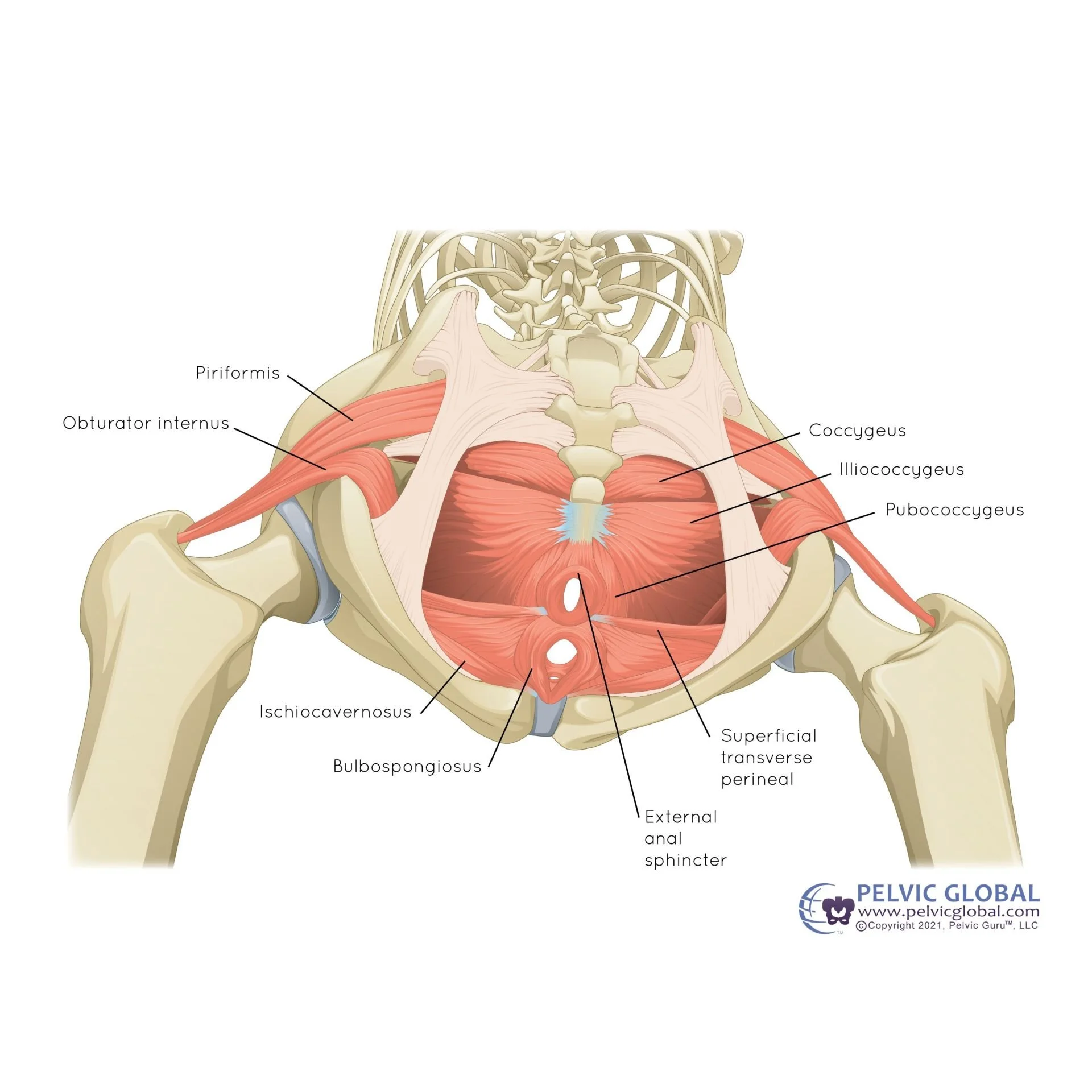
Some of the most common musculoskeletal causes of pelvic pain are tight, immobile, and hypersensitive pelvic floor muscles. The muscles that may contribute are the obturator internus, piriformis, bulbopongiosus, ischiocavernosus, coccygeus, and levator ani (puborectalis, pubococcygeus, and iliococcygeus). Muscle pain usually feels dull, achy, deep, but can sometimes be sharp. Common triggers for muscular pelvic pain are direct pressure (i.e. sitting), when actively using the muscles (i.e. exercise, bladder or bowel evacuation, sexual activity, etc.), or during times of increased nervous system activity (i.e. stress, anxiety, etc.).
The obturator internus, piriformis, or the pudendal nerve can cause pain with sitting, pain with physical activity (squats, etc), changes in bowel, bladder, or sexual function. Pain from the obturator internus (OI) muscle usually presents just to the inside of the butt bones (SITS bones). It can often be mistaken for piriformis syndrome or proximal hamstring tendinitis. The OI is located a bit lower down than the piriformis, and a bit higher up than the proximal hamstring. It is located more medial and inside the pelvis compared to both of those other muscles (see images below). The OI and deep hip rotators act as secondary hip stabilizer muscles. When the primary hip stabilizers (core, low back, and glutes) are not strong enough to support you during activity, your secondary stabilizers kick in. We want this to happen, but if you are already prone to pelvic floor muscle tension & hypersensitivity, PLUS the OI is getting turned on to stabilize your hip, the muscles NEVER get a break. Then they become painful because they’re overworked and irritated.
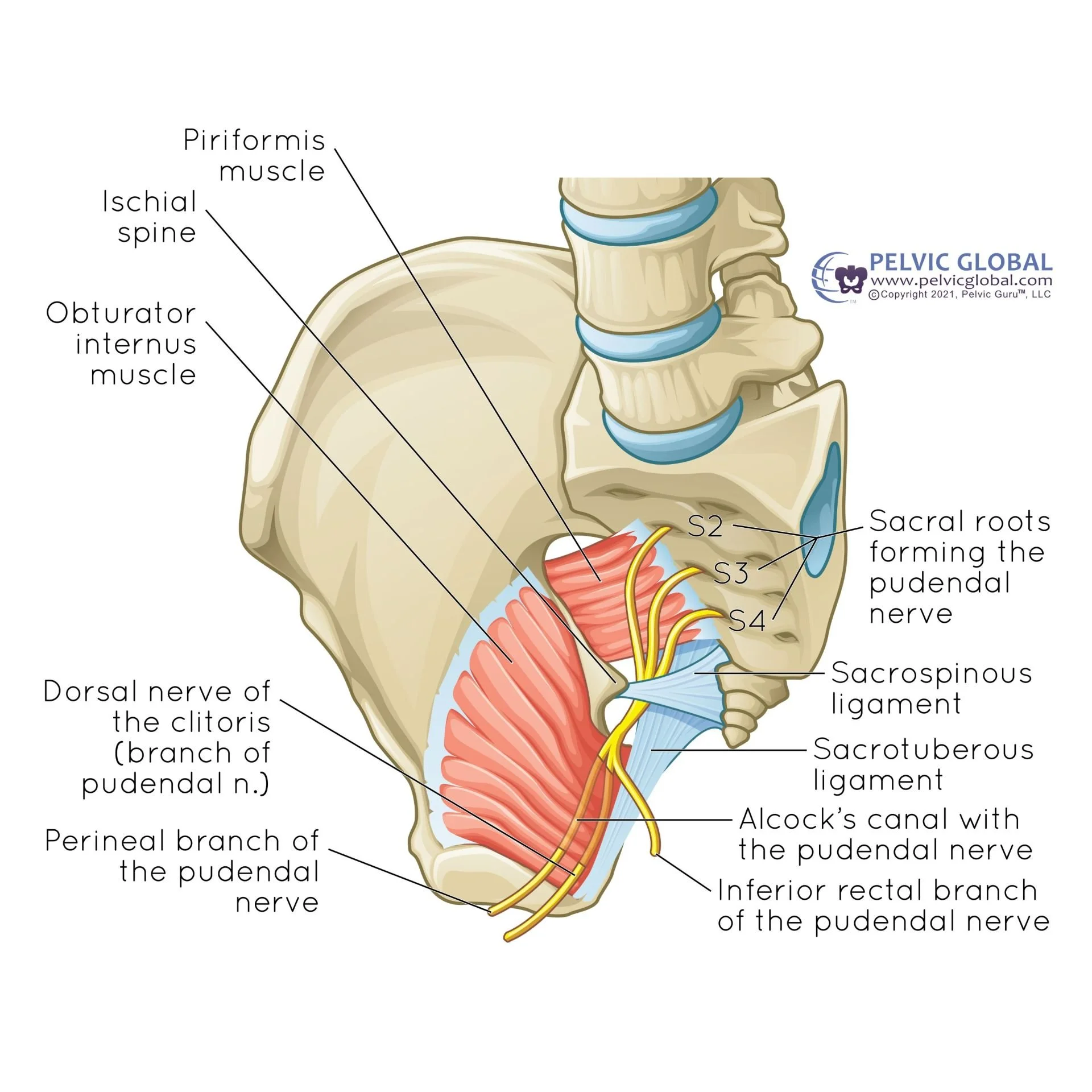
However, the OI and piriformis can both contribute to pelvic nerve irritation, especially the pudendal nerve pathway. If the OI or piriformis are tight, irritated, or if the nerve is entrapped by scar tissue, it can cause issues. The pudendal nerve (PN) provides motor, sensory, and autonomic innervation to the pelvic region. It plays a crucial role in urinary and bowel continence, sexual function, and genital sensation.The PN starts at the sacral nerve roots S2-S4, exits through the greater sciatic foramen (just under the piriformis), and wraps around the ischial spine and the sacrospinous ligament. It re-enters the pelvis and perineum through the lesser sciatic foramen and then through Alcock’s canal. Finally, it splits into three branches:
Inferior rectal branch: Innervates the external anal sphincter and perianal skin.
Perineal branch: Innervates the muscles of the perineum and skin of the scrotum or labia.
Dorsal branch to the penis/clitoris: Provides sensory innervation to the glans
Improving these issues can be a long journey, but it’s not impossible. Doing pelvic floor muscle lengthening, improving hip mobility, and strengthening the primary hip stabilizers can help manage your symptoms and even get you pain-free. It’s important to get your own pelvic rehab provider to do an assessment to determine the cause of your pelvic symptoms. But I typically suggest patients start with exercises like:
https://www.instagram.com/p/DWht1p0Ebl-/
https://www.instagram.com/p/DYDX56kR4AF/
https://www.instagram.com/p/DYscqCHOb5x/
1st image below: “Hemipelvis, Pudendal Nerve, Alcock's Canal”
2nd image below: “Inferior View, Rotators, Pelvic Floor”